




K. Luxová, T. Novotný, L. Koc, J. Ničovský, A. Tomášek, L. Křikavová, P. Kala
Souhrn
Perzistující foramen ovale se v naší populaci vyskytuje přibližně u 20 % dospělých lidí. Bývá spojováno s rizikem vzniku paradoxní embolie, kdy se trombus dostane přes zkrat do systémového řečiště. Trombus se může zaklínit ve foramen ovale. Je to vzácný stav spojený s vysokou mortalitou, důležitá je včasná diagnostika a zahájení terapie. V kazuistice popisujeme 37letou ženu s trombem zaklíněným ve foramen ovale, bilaterální masivní plicní embolií a paradoxní embolizací do arterií obou dolních končetin. V současné době neexistují jednotná doporučení ohledně terapie. Dle dostupných kazuistik a review je u trombu zaklíněného ve foramen ovale preferována chirurgická trombembolektomie, eventuálně dle stavu pacienta trombolytická či antikoagulační terapie.
© 2024, ČKS.
Klíčová slova:
Abstract
Patent foramen ovale occurs in up to 20% of adults and is associated with a higher risk of paradoxical embolization when a thrombus enters the systemic circulation through a shunt. The thrombus can also wedge in the foramen ovale. It is a rare condition associated with high mortality, and early diagnosis and treatment are essential. In this case report, we present a 37-year-old woman with a thrombus entrapped in the foramen ovale with bilateral massive pulmonary embolism, and paradoxical embolization to the arteries of both lower extremities. There are no uniform guidelines regarding therapy. According to available case reports and reviews, surgical thrombectomy for a thrombus entrapped in the foramen ovale is preferred. Depending on the patient’s condition, thrombolytic or anticoagulant therapy may be considered.
Keywords:
Address: MUDr. Kateřina Luxová, Department of Internal Medicine and Cardiology, the University Hospital Brno, Jihlavská 20, 625 00 Brno, the Czech Republic, e-mail: luxova.katerina@fnbrno.cz
Please cite this article as: Luxová K, Novotný T, Koc L, et al. Biatrial Thrombus Entrapped in Patent Foramen Ovale: An Acute Condition Requiring Early Diagnosis and Therapy. Cor et Vasa Case Reports 2024;7:15–18.
Patent foramen ovale (PFO) occurs in up to 20% of adults.1,2 It is a risk factor for paradoxical embolization when the thrombus reaches the systemic circulation through a shunt. A thrombus present in the right heart is called a “thrombus in transit”. If it is floating and not attached to the cardiac tissue, it is associated with a high risk of fragmentation and embolization.3,4 In acutely elevated pulmonary artery pressure, a foramen ovale can become patent and allows the thrombus to migrate towards the left atrium, producing paradoxical systemic embolization. If the thrombus is sufficiently large in comparison with the size of the PFO, it can become trapped there.2,5–7 This condition is associated with high mortality and requires immediate intervention.5
A 37-year-old woman was admitted to the emergency department for sudden shortness of breath and paresthesia in her lower extremities. She had suffered a fibula fracture six weeks ago, and she was on hormonal contraceptives. Otherwise, she was healthy.
She was taking a prophylactic dose of low molecular-weight heparin, which she had discontinued one week before. On arrival at the hospital, she had resting dyspnea, sinus tachycardia (100/min), and normotension (130/95 mmHg). Auscultation findings on her lungs were normal, while pulses were absent on both lower extremities. Electrocardiography (ECG) showed SI, QIII, and TIII patterns, and mild sinus tachycardia. She had a high level of D-dimer in her blood sample.
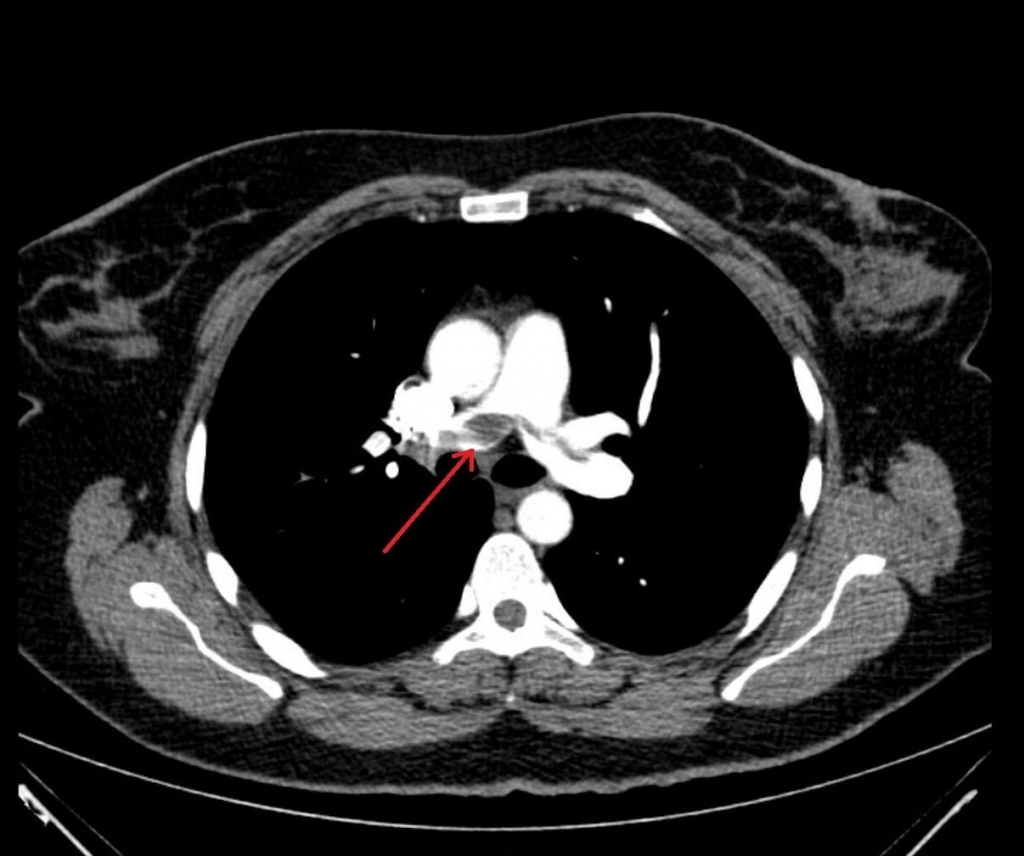
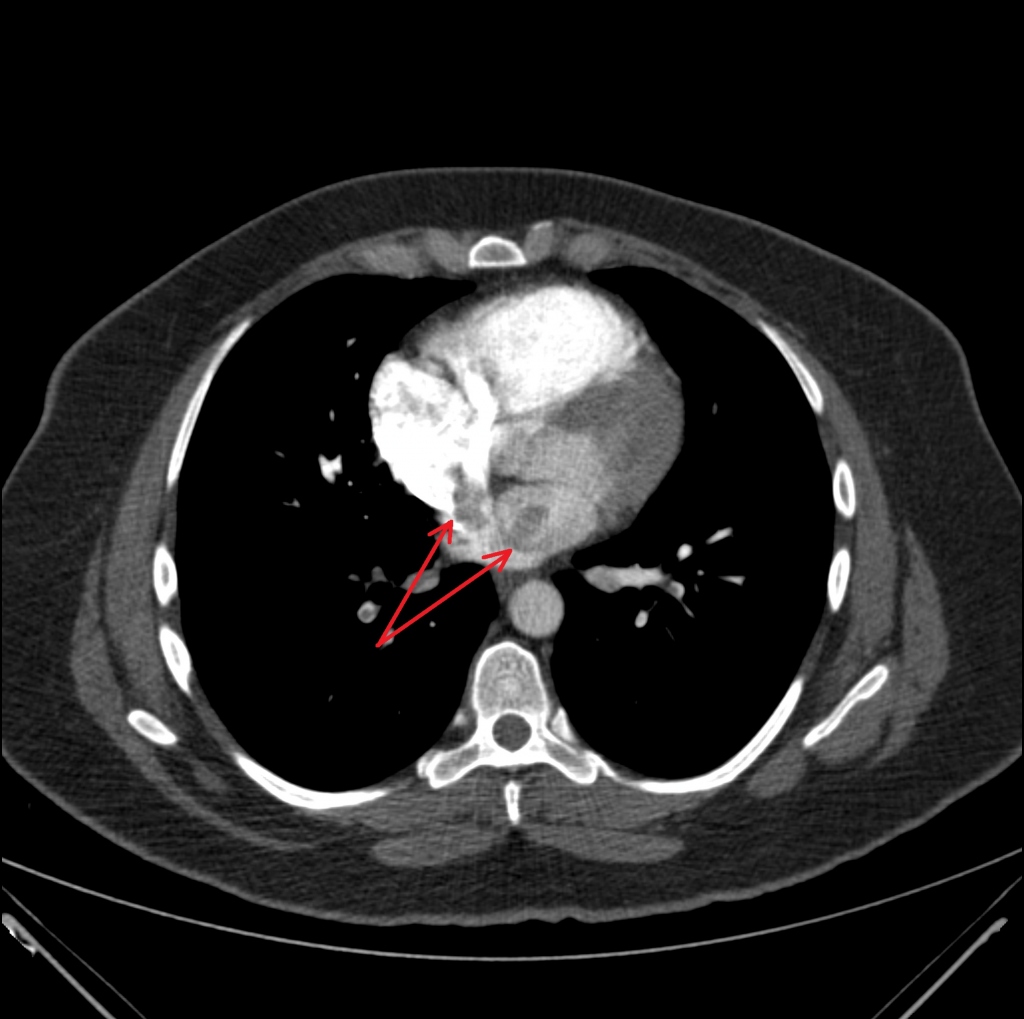
On the computed tomography angiography (CTA), bilateral pulmonary embolism (PE) with a massive fluttering thrombus in the pulmonary artery (Fig. 1) was found, and a thrombus in the left atrium was suspected (Fig. 2).
CTA of the lower limbs showed occlusion of the left common iliac and femoral arteries and occlusion of the right popliteal artery (Fig. 3) as possible signs of paradoxical embolization.

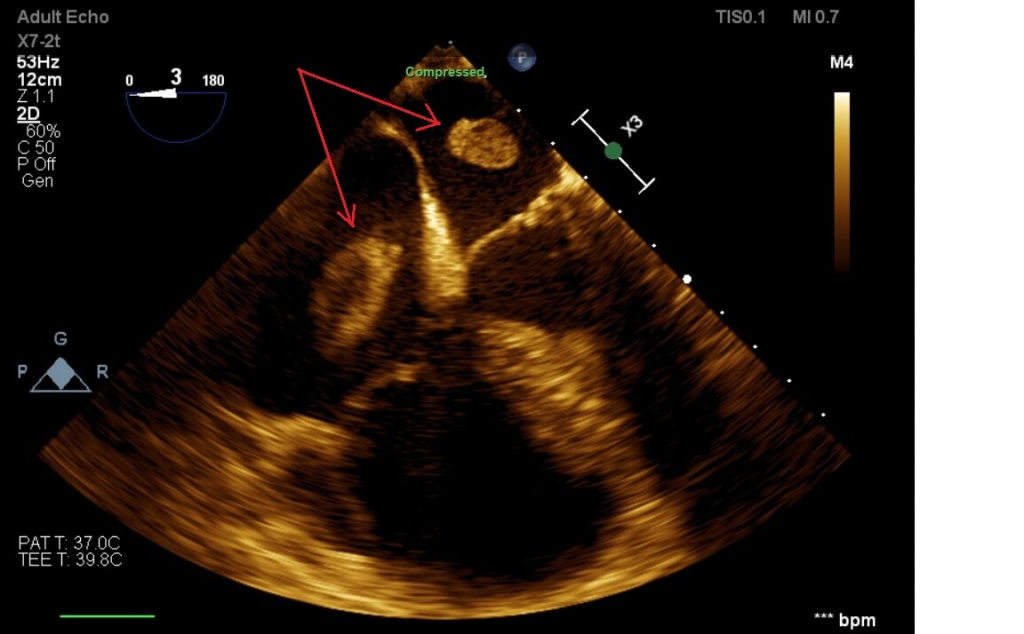
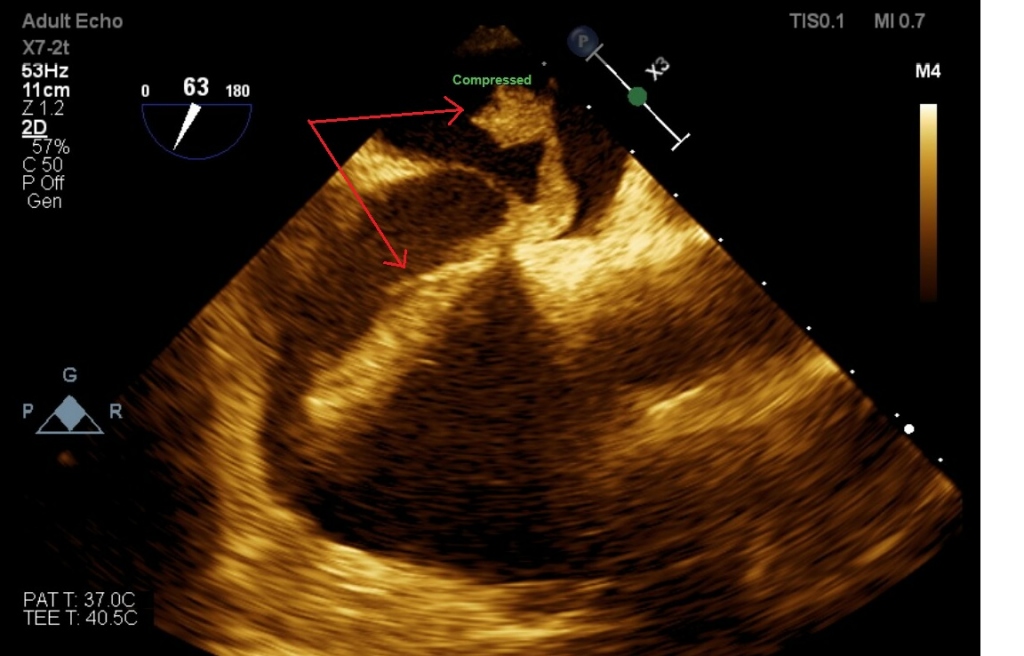
Deep vein thrombosis (DVT) in the left femoral and popliteal vein was found. Echocardiography revealed cor pulmonale with a large serpentine thrombus entrapped in the foramen ovale with a length of 80 millimeters fluttering in the right and left atria (Figs 4, 5). The findings were immediately consulted with the cardiac surgeon and it was decided to perform surgery.
In the operating theater, embolectomy of the pulmonary artery, removal of the entrapped thrombus, PFO suture, and embolectomy from the lower extremities were performed (Fig. 6).

In the postoperative period, the patient was temporarily on a low dose of vasopressors with a favorable postoperative outcome. After surgery, there was a reduction in dilatation and an improvement in the systolic function of the right ventricle. The patient was tested for thrombophilias, which were not proven. She was discharged home in a good condition and used warfarin anticoagulation for 1 month, followed by apixaban for 1 year. In the 4-year follow-up, she was without thrombosis recurrence and without posttrombotic syndrome.
We are presenting a case report of an acute and rare medical condition – a thrombus entrapped in the foramen ovale patent with signs of paradoxical embolism. From the very beginning, the combination of symptoms of PE and lower limb ischemia were suggestive of paradoxical embolization.
Lower limb fracture is a strong provoking factor for venous thromboembolism (VTE). Other strong provoking factors are hospitalization for heart failure or atrial fibrillation/flutter, hip or knee replacement, major trauma, myocardial infarction, previous VTE, and spinal cord injury. Estrogen-containing oral contraceptives are associated with a moderate VTE risk.8 Oral contraceptives increase the risk of VTE 3–4 times.9
In the diagnostic algorithm, the first-line investigation is ECG recording (as it is widely available), although it is neither sensitive nor specific for PE diagnosis. A normal ECG can be seen in 30% of patients with PE.10 Nevertheless, in our case it showed the SI, QIII, TIII pattern typical for PE.11 Currently, pulmonary artery CT angiography is considered the first-choice diagnostic imaging technique in patients with suspected PE with high sensitivity and specificity.12
After confirming PE and peripheral arterial embolization, an arteriovenous shunt was suspected. Therefore, echocardiography was performed and an embolus entrapped in the foramen ovale was found. Echocardiography is the leading method in diagnosing intracardiac thrombi and shunts. Transesophageal echocardiography is a more specific method which can image a thrombus more accurately and assess flow through PFO.3,4,13
The origin of the thrombus was deep vein thrombosis. Most pulmonary emboli and right heart thrombi originate from clots forming in the deep veins of the lower extremities.5 PE occurs with most episodes of symptomatic proximal DVT.14
Finding free-floating thrombi in the right heart is a rare condition, often associated with acute pulmonary embolism and increased mortality. In 3–23% of pulmonary embolism cases, intracardiac thrombus is present.5 Chartier et al. reported a 44.7% mortality rate during hospitalization in their study of 38 patients with a thrombus in the right heart. Of these, 8 (21%) died within the first 24 hours.13 The incidence of biatrial thrombi is unknown. It is an extremely rare condition which has been reported in only a few case reports.3–5,7,15
After diagnosing an entrapped embolus in the foramen ovale, our patient was sent to the cardiac surgery department for emergency surgical treatment. The therapy of patients with biatrial thrombus and paradoxical embolization is controversial, and there is no universally accepted consensus. The therapeutic options proposed in the literature are anticoagulation, thrombolysis, percutaneous thrombectomy, and surgical embolectomy.3,15 If the thrombus is biatrial with paradoxical embolization, most authors recommend surgical thromboembolectomy with closure of the foramen ovale because of the high risk of systemic embolization during thrombolysis or heparinization.2,4,6,16 According to a review of 174 patients by Myers et al., surgical thrombembolectomy showed a nonsignificant trend towards lower mortality and significantly reduced systemic embolization, compared with anticoagulation alone.6 A recent review by WW Seo et al. showed that surgical management is associated with a lower 60-day mortality.16 Surgical management has shown lower mortality and risk of embolization to the system circulation in patients with biatrial thrombus and paradoxical embolization.5,6,16 However, in patients in cardiogenic shock, there was no difference in mortality in patients treated with thrombolysis, anticoagulation, or surgery.16 Surgical management is preferred in hemodynamically stable patients instead of thrombolysis, which should be considered in hemodynamically unstable patients in cardiogenic shock.16 Heparinization is not recommended as a stand-alone therapy because of the high mortality rate (up to 60%), although it may eventually be used in stable patients.13 Percutaneous intervention is a promising option. However, so far, we need more evidence of its outcomes.5
Biatrial thrombus with paradoxical embolization is a rare condition which is associated with high mortality. Early and correct diagnosis is essential. An echocardiographic examination is the most appropriate method for diagnosis. There is no clear consensus on therapy. In biatrial thrombus entrapped in the PFO with a risk of paradoxical embolization, surgical management is preferred.
Acknowledgements
The language correction was done by Beau Daquila.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by MH CZ – DRO (FNBr, 65269705).
Ethical statement
I declare on behalf of all authors that the research was conducted according to the Declaration of Helsinki.
Informed consent
The authors declare that informed consent was obtained from the patient.
References
MUDr. Kateřina Luxová graduated from the Faculty of Medicine of Masaryk University in 2018. After finishing her studies, she started to work at the Department of Internal Medicine and Cardiology in the University Hospital Brno. Since then she has worked at the Department and has improved her abilities gradually. She has been interested in the field of acute cardiology and arrhythmology, in which she specializes in her PhD studies as well.



