




N. Seredyuk, O. Babliak, A. Vytrykhovskyi, R. Petrovskyi, A. Matlah, Y. Vandzhura, O. Tsaruk, I. Grabas, O. Skakun, M. Bielinskyi, I. Tverdokhlib, M. Serediuk
Abstract
Anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA), also called Bland–White–Garland syndrome, is a rare congenital coronary artery abnormality that often manifests itself by chronic myocardial ischemia, angina during breastfeeding, myocardial infarction, sudden cardiac death. This article reports on the ALCAPA in an adult man. The patient complained of chest discomfort for a long time, a silent myocardial infarction was suspected. When he was 29 years old, he developed out-of-hospital cardiac arrest while exercising (treadmill at the gym) with successful electrical cardioversion and resuscitation. ALCAPA diagnosis was verified using computed tomography coronary angiography (CTCA). Left anterior minimally invasive thoracotomy was performed. Left coronary artery (LCA) trunk was ligated, cut, and sewed, distal LIMA-LAD anastomosis was made. Two weeks after the surgical correction a postpericardiotomy syndrome developed, which was successfully treated using methylprednisolone and ibuprophene.
© ČKS, 2022.
Keywords:
ALCAPA
Left coronary artery
Myocardial infarction
Postpericardiotomy syndrome
Pulmonary artery
Sudden cardiac death
Surgical correction
Address: Prof. Nestor Seredyuk, MD, National Medical University and Regional Clinical Cardiology Center, Ivano-Frankivsk, Ukraine, e-mail: seredyuknestor@gmail.com
Please cite this article as: Seredyuk N, Babliak O, Vytrykhovskyi A, et al. Anomalous origin of the left coronary artery from the pulmonary artery as a life-threatening condition. Cor et Vasa Case Reports 2022;5:15–17.
Anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA or Bland–White–Garland syndrome) is a rare congenital heart anomaly with an incidence of 1 in 4243 live births or 0.023%.1 About 10–15% of all cases are diagnosed in adult age.2 There are two types of this syndrome: an infantile type that is characterized by poor collaterals between the left coronary artery (LCA) and the right coronary artery (RCA), and adult type in which collaterals are well-developed.3,4 Symptoms of ALCAPA in adults include angina, myocardial infarction, papillary muscle calcification, endocardial fibroelastosis, mitral regurgitation, heart failure.3,5 Chronic myocardial hypoperfusion often leads to the dilation of the left ventricle and reduced contraction of its walls resulting in a decrease in the left ventricular ejection fraction.6
A 29-year-old patient K. was asymptomatic in childhood. The heart murmur was detected when the patient was 15 years old. ECG and echocardiography were performed and no pathological changes were found. Later left-sided chest discomfort appeared. Repeated ECG and echocardiography showed no pathological changes. The patient finished medical university and became a dentist.
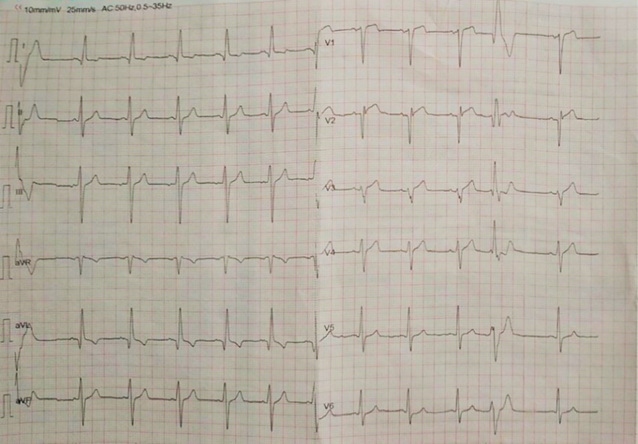
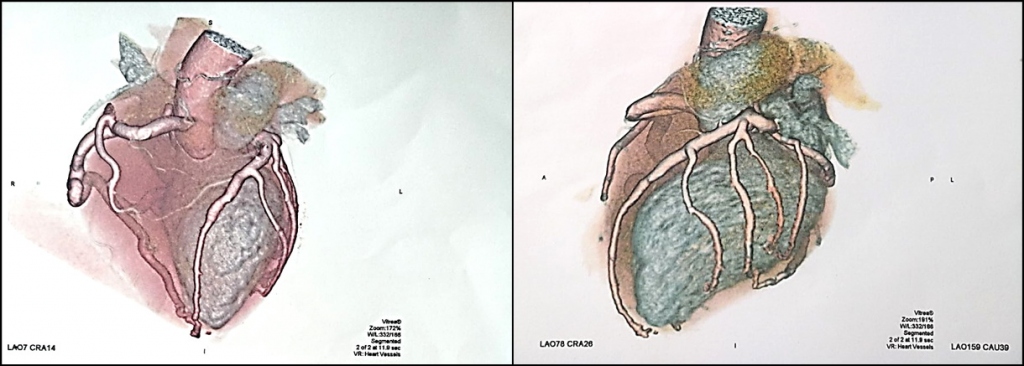
The patient suddenly developed ventricular tachycardia/ventricular fibrillation during exertions on the treadmill at the gym. Prompt resuscitation was started, consequent two defibrillation procedures were performed and sinus rhythm was restored. On a12-lead ECG performed after resuscitation a sinus rhythm with ventricular extrasystoles is seen, probably signs of previous antero-septal myocardial infarction (qR in I, avL; Qr in V2), ST elevation in V1–V3, signs of left ventricular hypertrophy (Fig. 1). CT coronary angiography revealed the origin of the LCA from the proximal segment of the pulmonary artery, recessive and convoluted RCA originated from the right Valsalva sinus (Fig. 2).
A left anterior mini-thoracotomy was performed. The left internal mammary artery was harvested. The left main coronary artery was tied with two ligatures and sewn. Coronary artery bypass grafting LIMA-LAD was performed. There was a normal early postoperative period. But in two weeks the patient developed a fever and tachycardia. Echocardiography revealed hyperechogenic pericardial effusion with a separation of the pericardial layers of 1 cm. PaO2 decrease to 92–94% was registered. The postpericardiotomy syndrome was diagnosed. Methylprednisolone (32 mg a day with gradual dose reduction by 2.5 mg every two weeks), ibuprophene (600 mg a day), bisoprolol (2.5 mg a day), aspirin (100 mg a day), clopidogrel (75 mg a day), indapamide (1.25 mg a day) were prescribed. There was normal recovery at follow-up at 1, 3, and 6 months, and the patient returned to work.
ALCAPA is a severe congenital heart anomaly. Its course may be unpredictable and dramatic, as described in this case. ALCAPA, rather than coronary atherosclerosis, resulted in a dramatic event. Left ventricular myocardium was receiving poorly oxygenated blood with high carbon dioxide content for a long time. For a certain period of time, collaterals between the LCA and the RCA provided myocardial viability, but exertions causing the imbalance between the myocardial oxygen demand and its delivery, has led to the type 2 myocardial infarction (according to the Fourth Universal Definition of Myocardial Infarction, ESC, 2018).7 Silent anteroseptal myocardial infarction was complicated by ventricular fibrillation and sudden clinical death. The imbalance between the oxygen delivery to the myocardium and its demand occurs in the case of ALCAPA.
In infants, ALCAPA is characterized by intermittent anxiety paroxysms, significant pallor, vomiting, significant sweating during breastfeeding (“breastfeeding angina”).8 Coronary artery aneurysm development can occur in ALCAPA patients.9 Episodes of chest discomfort in this patient were considered with some skepticism which almost brought him to a fatal outcome.
This case supports an opinion, that ALCAPA is not only a theoretical problem but also a serious problem in real clinical practice. Most cardiac symptoms of ALCAPA are caused by impaired metabolism due to chronic myocardial hypoxia. The imbalance between oxygen delivery and myocardial demand significantly increases upon exertions. It’s the background for the development of chronic coronary syndrome, myocardial infarction, sudden cardiac death. Coronary angiography and CT coronary angiography, both are reliable methods for the establishment of the ALCAPA diagnosis.10,11 Ligation and sewing of the left main coronary artery near its origin from the pulmonary artery and coronary artery bypass grafting LIMA-LAD is an effective method of the surgical correction of the ALCAPA.
ALCAPA is a congenital coronary artery anomaly that can be diagnosed not only in children but in adults as well. This anomaly may lead to myocardial infarction and sudden cardiac death. So, early diagnostics of this condition is very important. Coronary angiography and CT coronary angiography are reliable methods for confirmation of the ALCAPA diagnosis. Early surgical correction may prevent severe complications. The possibility of the postpericardiotomy syndrome should also be kept in mind, which requires timely pharmacological treatment (methylprednisolone).
Conflict of interest
None.
Funding body
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Ethical statement
I declare on behalf of all authors that the research was conducted according to the Declaration of Helsinki.
Informed consent
I declare on behalf of all authors that informed consent was obtained from all patients participating in this study.
References
Prof. Nestor Seredyuk, MD, head of the Department of Internal Medicine №2 and Nursery, Doctor of Medical Sciences, Professor, Vice-Rector for Research at Ivano-Frankivsk National Medical University (1987–2011 pp.), Head of the Department from 1987 to 2011 and from 2018 to present time, Honored Worker of Science and Technology of Ukraine, member of ASH (the American Society of Hypertension), member of ESC (the European Society of Cardiology).



