INVASIVE VALIDATION OF H2FPEF SCORE FOR DIAGNOSIS OF HEART FAILURE WITH PRESERVED EJECTION FRACTION (HFPEF)
Background: The diagnosis of heart failure is hemodynamically defined as an inappropriate elevation of filling pressures at rest or during exercise. The diagnosis of HF with preserved ejection fraction (HFpEF) remains challenging. Recently established H2FPEF score facilitates the diagnosis of HFpEF; however, there are only limited studies correlating this score with invasively measured LV filling pressures.
Methods: A cohort of 223 patients (age: 60 ± 10 years, 65% males) with LV ejection fraction ≥50%, symptoms attributable to HFpEF and nonvalvular atrial fibrillation (AF), scheduled for AF ablation were analysed. Mean left atrial pressure (mLAP) was measured at the beginning of the AF ablation procedure at rest and upon 3-min isometric handgrip exercise. HFpEF was defined invasively as the elevation of mLAP ≥15 mmHg at rest or ≥25 mmHg during handgrip.
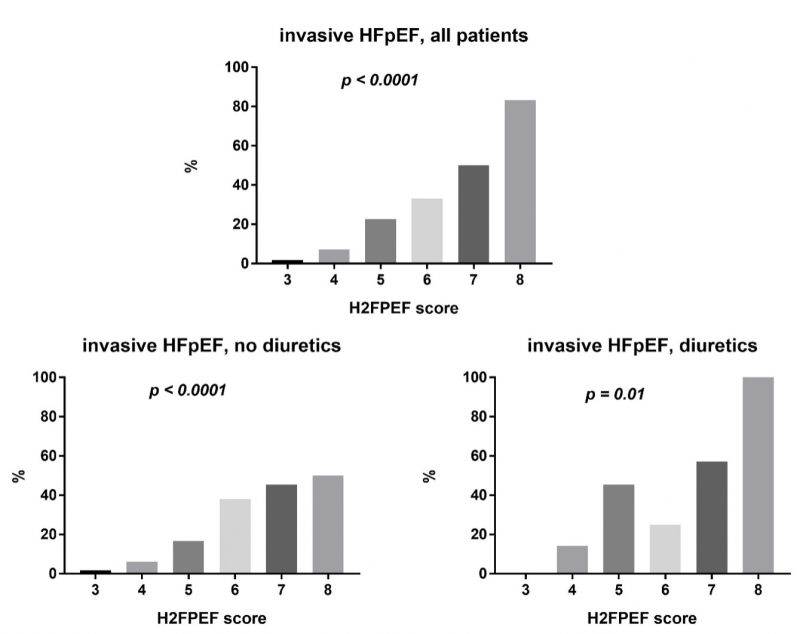
Results: Mean LAP progressively increased with increasing HF2PEF score (p<0.0001). However, the rate of HFpEF was much lower than originally reported, for example, ~50% instead of ~95% in patients with the H2FPEF score of 7. Patients taking diuretics (n= 44) had higher mLAP both at rest (12.0 ± 6.6 vs. 9.0 ± 4.6 mmHg, p= 0.0005) and during exercise (16.6 ± 9.1 mmHg vs. 11.9 ± 6.5, p= 0.0001), and had also more often HFpEF (38.6% vs. 14.0%, p= 0.0004). A cut-off value of ≥5 in patients without diuretics had the sensitivity of 84.0% and specificity of 66.3%; a cut-off value of ≥7 in patients with diuretics had the sensitivity of 47.1% and specificity of 64.3%. H2FPEF score overestimated the diagnosis of HFpEF in our cohort and offered only moderate sensitivity and specificity for the HFpEF prediction. The performance of H2FPEF was particularly poor in patients on diuretic therapy.