MORTALITY IN HYPERTROPHIC CARDIOMYOPATHY IS INDEPENDENT OF GENOTYPE
Background: Hypertrophic cardiomyopathy (HCM) patients with a pathogenic mutation are considered at greater risk of HCM-related adverse events (AE) than patients without the pathogenic mutation. Nevertheless, the relationships between genotype status and outcome have not been entirely resolved.
Methods: Consecutive patients (n=1468) with HCM diagnosis underwent genetic testing focused on HCM-related genes. Patients with pathogenic or likely pathogenic (P/LP) variants were considered genotype positive (G+), and those without P/LP variants or a variant of uncertain significance (VUS) were considered genotype negative (G-). Patients were followed for 9.6 ± 8.2 years for clinical outcomes.
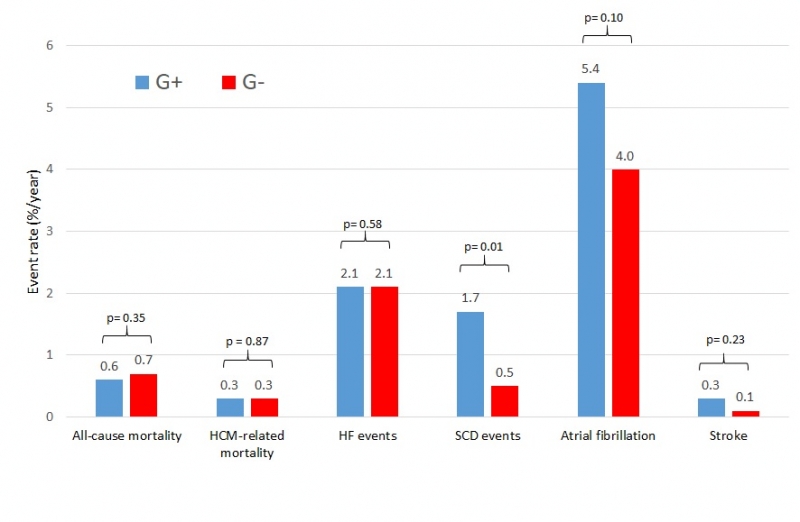
Results: Of 1468 HCM patients, 1156 (79%) were G - and 312 (21%) were G+. Over the follow-up, 135 (9%) patients died, including 33 (2%) from HCM-related causes (sudden death, embolic stroke, heart failure, surgery: heart transplant or myectomy). Sudden death events (appropriate ICD shocks, aborted cardiac arrest, and sudden death) were more frequent in G+ patients (1.7%/year) than in G- patients (0.5%/year) (HR 1.94; 95% CI 1.21-3.11; p=0.01). All-cause mortality was higher in G- patients compared to G+ patients (0.8%/year vs. 0.3%/year; p< 0.01), but after age adjustment, it did not differ between the groups (0.7%/year G- vs. 0.6%/year G+; p=0.35). HCM-related mortality was similar between G- vs. G+ HCM patients (0.3%/year vs. 0.3%/year; p=0.87). In multivariable analysis, age at diagnosis was an independent predictor of all-cause and HCM-related mortality (p<0.0001 for both), HF and SD events (p= 0.03 for both), while genotype was not. Conclusions: In this large consecutive genotyped cohort, all-cause and HCM-related mortality was unrelated to genotype status.