EFFECT OF ACUTE CELLULAR REJECTION AFTER HEART TRANSPLANTATION
Purpose: In patients after heart transplantation the role of moderate acute cellular rejection(Banff 2) without clinical and echocardiographic manifestation is not yet clear. We evaluated the course of the first two posttransplantation years in relation to rejection episodes.
Methods: this is a retroprospective study of one hundred thirty-nine heart transplant recipients who were operated between January 2000 and December 2004 and survived first 6 months. We analyzed the presence of acute rejection during first 6 months in relation to the course of the first two postoperative years.We observed graft dysfunction, incidence of infections, malignancy, immunosuppressive therapy and mortality.According to the degree of cellular rejection, patients were divided into groups: 1- without the presence of significant cellular rejection (№ 67), 2 - with only one episode of acute cellular rejection Banff 2: 2a -who received acute antirejection treatment (№ 19), 2b - who didn't receive acute antirejection treatment (№ 8), 3 – with repetitive occurrence of rejection Banff ≥ 2 (№ 45).
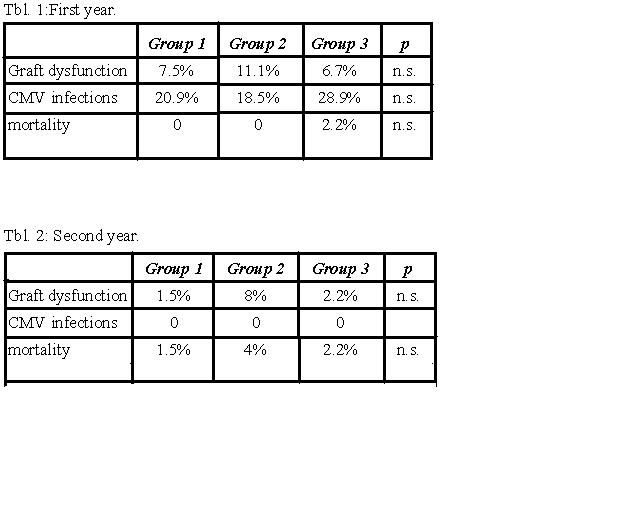
Results : We didn't observe statistically significant differences in monitored parameters among the three groups(see tbl.1, 2). The main change in immunosuppresive therapy was conversion from cyclosporin A(CsA) to tacrolimus (Tac) during the follow-up. The significantly higher Tac using was detected at the first and second years after transplantation ( gr. 3 – 31.8%, gr. 2 – 16%, gr. 1.- 10.6% 3:1 p <0.001, 2:1 p <0.031).
Conclusions: We didn't prove a significant impact of moderate cellular rejection on course of the first two years after heart transplantation. The high incidence of recurrent rejection is an indication for the conversion from CsA to Tac.